
Ovarian Torsion: An Evidence-Based, Patient-Centered Guide for Clinical Reality, Recovery, and Awareness
- Feb 16
- 14 min read
Updated: Feb 23
Summary
What it is. Ovarian torsion (often called adnexal torsion) is twisting of the ovary, and sometimes the fallopian tube, around its supporting ligaments and vascular pedicle, which can reduce or cut off blood flow (ischemia). It is a true surgical emergency because prolonged ischemia can lead to loss of ovarian function, tissue necrosis, infection, and (rarely) life-threatening complications if untreated. [1]
What it feels like. The classic picture is sudden, severe one-sided lower abdominal/pelvic pain, commonly with nausea/vomiting. Pain can also be intermittent (twist–untwist), which contributes to delays and misdiagnosis. [2]
How it’s diagnosed. Ultrasound (with Doppler) is the first-line imaging test, but torsion is ultimately a surgical diagnosis. Importantly, normal Doppler flow does not rule out torsion (e.g., 61% of right-sided torsions and 27% of left-sided torsions had normal Doppler flow in one study). [3]
How it’s treated. Standard care is urgent surgery, usually laparoscopy, to untwist the adnexa (detorsion) and address the cause (often cystectomy). Contemporary guidance emphasizes ovarian preservation whenever feasible, even when the ovary looks very dark, because appearance alone is an unreliable predictor of viability. Removal (oophorectomy/salpingo-oophorectomy) is generally reserved for clearly nonviable tissue or other unavoidable circumstances. [4]
Fertility after losing one ovary. Many people still ovulate, menstruate, and conceive with a single ovary. However, population studies suggest menopause may occur modestly earlier on average (roughly ~1–2 years) after premenopausal unilateral oophorectomy, particularly when the surgery occurs at younger ages. Ovarian reserve (quantity) may be reduced, while egg/embryo quality may be less affected, important for counseling, especially if fertility treatment is needed later. [5]
A note on scope. This is educational content, not medical advice. If you suspect torsion, treat it as an emergency and seek urgent care. [6]
What ovarian torsion is and why it is time-sensitive
Definition. Ovarian torsion is twisting of the ovary on its ligamentous supports; “adnexal torsion” is broader and includes torsion of the ovary and/or fallopian tube. The torsion compresses blood vessels and can reduce perfusion. [1]
Pathophysiology in plain language.
The twist first impairs venous and lymphatic outflow, producing congestion and swelling (edema).
As swelling worsens, arterial inflow becomes compromised, leading to ischemia and potentially infarction/necrosis if not corrected. [7]
Why imaging can be misleading. Because the ovary has a dual blood supply and torsion may be partial or intermittent, Doppler flow can still appear present. This is why clinical suspicion matters and why “normal Doppler” cannot safely rule out torsion. [8]
Time matters, but the exact clock is uncertain. There is no universally agreed “hours-to-necrosis” threshold. Data are mixed: some series find symptom duration correlates with ovarian loss, while others show salvage can still be possible despite prolonged symptoms. In one pediatric study, ovarian loss correlated with longer symptom duration (24 vs 96 hours), while time from diagnosis to surgery was not significantly different. [9] In another pediatric cohort, prolonged symptoms did not preclude salvage, and the authors stressed urgent imaging and management. [10] Real-world ED series also report that ovaries may remain viable even after longer symptom durations in some cases, reinforcing that the safest approach is urgent evaluation whenever torsion is suspected. [11]
How common it is and who is at risk
Epidemiology (what we can say with confidence). True population incidence is hard to pin down, but multiple reputable sources describe torsion as a relatively uncommon but important emergency. It has been described as the fifth most common gynecologic emergency and is often discussed as accounting for a small percentage of gynecologic surgical emergencies. [12] One ED-based study estimated incidence around 157 per 100,000 ED visits among reproductive-age women in that setting. [13]
Who it tends to affect. Most cases occur during reproductive years, but torsion can occur at any age (including children and postmenopausal patients). [14]
Risk factors (the big ones).
Ovarian cysts or benign masses are the most common drivers; risk rises with larger size (often cited at ≥5 cm). [15]
Pregnancy, particularly with corpus luteum cysts; Cleveland Clinic notes about 1 in 4 diagnosed are pregnant (a clinical estimate that varies by study). [16]
Fertility treatment/ovulation induction (enlarged, stimulated ovaries). [17]
Prior torsion, which increases recurrence risk. [18]
Longer-than-average ligaments or increased mobility (anatomic predisposition). [19]
Benign vs malignant masses. Torsion is more commonly associated with benign lesions than malignancy in reported series. [20]
How it presents and what else it can be
Core symptoms.
Red flags that should prompt urgent ED evaluation.
Diagnostic comparison table: torsion vs common mimics
Condition | Pain pattern | Common associated symptoms | Helpful clues | First tests that matter most |
Ovarian torsion | Sudden severe unilateral pelvic/lower-abdominal pain; can be intermittent | Nausea/vomiting common | Known ovarian cyst/mass; reproductive age; pregnancy or ovulation induction risk | Pregnancy test, pelvic US (with Doppler) to support suspicion—but surgery confirms [24] |
Ruptured ovarian cyst | Sudden pain often after activity/intercourse; may improve over hours | Light vaginal bleeding, nausea possible | Free fluid; pain may be more self-limited | Pregnancy test; pelvic US [25] |
Ectopic pregnancy | Pelvic pain (may be unilateral), can be sharp | Vaginal bleeding, dizziness/syncope | Positive pregnancy test; risk factors (prior ectopic, PID) | Pregnancy test + urgent pelvic US [23] |
Appendicitis | Migratory pain to RLQ; progressive | Fever, anorexia, nausea | Rebound/peritoneal signs; leukocytosis may occur | CBC; CT/US based on setting; surgery consult if high suspicion [23] |
PID / tubo-ovarian abscess | Gradual pelvic pain; bilateral common | Fever, discharge, dyspareunia | Cervical motion tenderness; STI risk | Pelvic exam; pregnancy test; labs; US if abscess suspected [26] |
Renal colic (kidney stone) | Flank pain radiating to groin; colicky | Hematuria, nausea/vomiting | Costovertebral angle tenderness | UA; CT KUB/US per protocol [25] |
Diagnosis in the real world: labs, imaging, and where CT/MRI fit
Clinical stance (important): torsion is not a “rule-out” diagnosis. ACOG emphasizes that there are no clinical or imaging criteria sufficient to confirm torsion preoperatively, Doppler flow should not drive decisions alone, and torsion remains a surgical diagnosis. [27]
Initial labs (typical ED workup).
Ultrasound (US): first-line imaging.
Transvaginal US is commonly used; supportive findings can include enlarged ovary, ovarian mass/cyst, peripheral follicles, free fluid, and sometimes the “whirlpool sign” of a twisted pedicle. [30]
Accuracy varies. In one study of surgically proven cases, US sensitivity was ~70% and specificity ~87%. [31]
Doppler: helpful, but dangerous if used as a “no torsion” stamp.
When CT is used (and what it can show). CT is often not the first imaging choice when torsion is suspected; however, in many EDs, CT is commonly obtained when the diagnosis is unclear or when GI/urinary causes are being evaluated. CT findings that can increase diagnostic certainty include ovarian enlargement, thickened tube, twisted pedicle, abnormal enhancement, engorged vessels, uterine deviation, ascites, and periadnexal fat stranding. [32]
When MRI is used (and why).MRI can be helpful when US is equivocal, when radiation avoidance is important, or when soft-tissue characterization is needed. MRI may show edema, hemorrhage, tubal thickening, ascites, uterine deviation, and lack of enhancement in necrosis; MRI is also often preferred over CT in pregnancy because it avoids ionizing radiation. [33]
Treatment, surgical choices, and fertility/hormonal implications
Decision principle: The goal is urgent detorsion and ovarian preservation when possible, because ovarian appearance can be misleading and function may return even after dramatic discoloration. [34]
Surgical options and tradeoffs
Surgical approach | What it is | Typical advantages | Typical downsides/risks | When it’s commonly chosen |
Detorsion (untwisting) | Untwist the ovary/adnexa to restore perfusion | Preserves ovarian tissue and potential fertility | Risk of persistent pain or necrosis if truly nonviable (rare); may need additional procedures | Standard of care when salvageable; recommended even if ovary looks dark [35] |
Cystectomy | Removal of the cyst (often the “lead point”) | Reduces recurrence risk; preserves ovary | Bleeding, adhesions; some impact on ovarian reserve depending on cyst type/technique | If a cyst/mass is present and ovary is viable [36] |
Oophorectomy / salpingo-oophorectomy | Removal of ovary (± tube) | Definitive treatment when tissue is nonviable or malignancy is suspected | Loss of half of ovarian reserve; potential earlier menopause; emotional impact | When ovary is clearly necrotic/nonviable or removal unavoidable [37] |
Oophoropexy | Fixation to reduce recurrence | May prevent repeat torsion in select cases | Limited evidence; not routine for first event in many settings | Recurrent torsion or special situations per clinician judgment [38] |
Laparoscopy vs laparotomy.
Fertility and hormones after unilateral oophorectomy (one ovary removed)
What most patients can expect. Many people maintain menstrual cycles and fertility potential with one ovary, because the remaining ovary can continue ovulation and endocrine function. Cleveland Clinic explicitly notes you can still get pregnant with one ovary. [41]
But counseling should include nuance.
Ovarian reserve (quantity) decreases after unilateral oophorectomy, which may reduce the number of eggs retrieved in IVF, even if pregnancy rates are not always dramatically different across studies. [42]
Population studies suggest a modest shift toward earlier menopause (approximately ~1 year earlier in one large Norwegian cohort; ~1.8 years earlier in a Danish cohort), and a recent community-based cohort found elevated risk of earlier natural menopause, particularly when unilateral oophorectomy occurred before age 40. [43]
If fertility goals are future-focused (or if you are already facing diminished reserve due to age/endometriosis/PCOS history), it may be worth discussing fertility planning (timelines, AMH/antral follicle count interpretation, and whether proactive consultation is appropriate). Evidence here is individualized rather than one-size-fits-all. [44]
Recovery, complications, and patient-centered planning
Perioperative care basics (what commonly happens)
Because torsion is usually urgent, the “pre-op optimization” window is short. Typical hospital steps include IV fluids, antiemetics, pain control, pregnancy testing in reproductive-age patients, and surgical evaluation. [45] Early mobilization and opioid-sparing pain strategies are common enhanced-recovery principles across surgeries; gynecologic ERAS pathways emphasize multimodal care, early feeding when safe, and early mobilization (though procedure-specific data vary). [46]
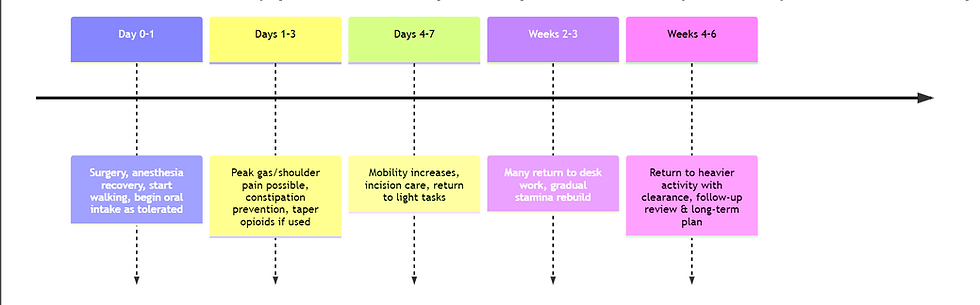
A realistic recovery timeline (laparoscopy is different from laparotomy)
Most torsion surgeries are laparoscopic; some are open. General timelines below assume laparoscopic detorsion/cystectomy or laparoscopic unilateral oophorectomy; open surgery often extends these ranges. [47]
Time window | What you may feel | What usually helps | Typical milestones (general guidance) |
Day 0–1 | Grogginess, abdominal soreness; shoulder-tip pain from laparoscopy gas is common | Scheduled acetaminophen/NSAIDs if safe; short walks; deep breathing | Many go home same day after laparoscopy; walking as tolerated [48] |
Days 1–3 | Gas/shoulder pain may peak; fatigue; constipation risk (esp. with opioids) | Movement, hydration, gentle diet; bowel regimen if opioids used | Incremental walking; pain and nausea should trend down [49] |
Days 4–7 | Less pain; incision tenderness; tired easily | Light activity pacing | Many return to light tasks; some return to desk work (variable) [50] |
Weeks 2–3 | Energy improves; occasional “twinges” with movement | Graded return to routine | Many return to work within 1–3 weeks after laparoscopy depending on job demands [51] |
Weeks 4–6 | Most symptoms resolve; stamina returns | Gradual exercise restart after clearance | Many return to full activity by ~2–4 weeks after oophorectomy; longer if open surgery or complications [52] |
Why shoulder pain happens (so patients don’t feel blindsided). Shoulder-tip pain after laparoscopy is common and is thought to result from diaphragmatic irritation and referred pain via the phrenic nerve; systematic reviews note it can last up to ~3 days in many cases, with variable incidence across studies. [53]
Mermaid timeline: recovery phases after laparoscopic torsion surgery
timeline Recovery phases after laparoscopic detorsion/cystectomy or unilateral oophorectomy
Common complications and red flags
Most patients recover well, but you should have a low threshold to contact your surgical team or seek urgent care for concerning symptoms.
Potential complications to know about (not exhaustive):
Seek urgent evaluation for: fever, escalating abdominal pain, fainting, heavy bleeding, chest pain/shortness of breath, leg swelling, or inability to keep fluids down. (These are general postoperative danger signs; your discharge instructions may add procedure-specific items.) [54]
Nutrition, hydration, supplements, and lifestyle before and after surgery (with evidence level)
Because torsion is usually emergent, “pre-op” is often limited. Still, lifestyle and nutrition matter for recovery and for reducing preventable complications (constipation, dehydration, poor wound healing).
Core nutrition message (moderate evidence, high plausibility). Adequate calories and especially protein support tissue repair and immune function during wound healing, and nutrition deficits are associated with poorer healing outcomes in broader wound literature. [57]
Practical food pattern: protein with each meal (eggs, fish, poultry, tofu/beans, yogurt), plus fruits/vegetables and whole foods as tolerated. [58]
Hydration supports recovery; multiple patient-facing resources recommend drinking fluids regularly unless your clinicians restrict fluids for another condition. [59]
Early eating after surgery (moderate evidence; context-dependent). Enhanced recovery pathways across many surgeries encourage early oral intake when safe, which is associated with faster GI recovery in multiple contexts; however, evidence quality varies by procedure type and patient factors. Follow your surgical team’s plan. [60]
Constipation prevention (good evidence for opioid-induced constipation management). If opioids are used, consider asking about a bowel regimen: stimulant laxatives (senna/bisacodyl) ± osmotic agents (polyethylene glycol) are commonly recommended approaches. Avoid self-starting if you have contraindications; confirm with your clinicians. [61]
Supplements (strong safety guidance; limited benefit evidence). Many supplements can increase bleeding risk or interact with anesthesia. The American Society of Anesthesiologists notes that anesthesiologists may advise stopping supplements about two weeks before elective procedures. In emergency surgery, disclose everything you take as soon as possible. [62]- Evidence for specific supplements to accelerate healing after routine surgery is mixed and often indirect; vitamin C and zinc have biological roles in healing, but RCT-quality evidence for surgical-wound benefit is limited. If you supplement, do so under clinician guidance. [63]
Lifestyle (strong evidence for smoking cessation; general surgical best practice). Smoking is broadly associated with poorer surgical outcomes and delayed healing; if you smoke, cessation support is one of the highest-yield interventions for future procedures. (If torsion prompted surgery, this is still relevant for any later operations.) [64]
Pain management: pharmacologic and nonpharmacologic (and faith-respecting care)
Pharmacologic (standard approach; individualized). Many post-op pathways use multimodal pain control (acetaminophen, NSAIDs if safe, and limited opioids when needed), plus antiemetics. Your contraindications (kidney disease, ulcers, anticoagulants, allergies) matter, so personalize with your clinicians. [65]
Nonpharmacologic (growing evidence base, generally low risk). Reviews support the role of nonpharmacologic strategies, education, physical therapy/movement, and psychological supports, within multimodal pain management, though effectiveness varies by intervention and patient. [66]
Movement: gentle walking can reduce stiffness, support bowel function, and reduce clot risk. [67]
Breathing/relaxation: short breathing practices can reduce the stress amplification of pain. [68]
Meditation/mindfulness: systematic reviews suggest meditation can reduce perioperative anxiety and sometimes pain, though more rigorous trials are needed. [69]
Spiritual support (faith-respecting note): For patients who are religious, prayer/spiritual coping may be meaningful; research on prayer and pain is mixed and often context-dependent, but it can contribute to coping and positive reappraisal for some individuals. [70]
Practical guidance for patients
When to seek care (decision rule). If you have sudden severe pelvic/lower-abdominal pain, especially with nausea/vomiting, or you know you have an ovarian cyst/mass: go to the ER immediately. The cost of delay can be loss of the ovary. [71]
Questions to ask your surgeon (high-yield).
“Were you able to detorse and preserve the ovary? If not, why was removal unavoidable?” [72]
“What did you find (cyst type, size)? Was cystectomy done?” [56]
“Do I need follow-up imaging (often around ~6 weeks in some practices) to confirm perfusion/follicles?” [73]
“What is my recurrence risk, and would oophoropexy ever be considered?” [56]
“How might this affect fertility planning, and should I see a reproductive endocrinologist?” [44]
What to pack or prepare for the ER (practical, not medical). Bring ID/insurance, a list of meds/supplements, last menstrual period date, pregnancy status if known, allergies, and a phone charger. If possible, avoid eating or drinking once severe symptoms begin because surgery may be needed urgently (follow ED instructions). [74]
Planning travel and work after torsion surgery.
Most people need at least 1–3 weeks to return to desk work after laparoscopy; physically demanding work typically requires longer and individualized clearance. [75]
Avoid long-haul travel until you can walk comfortably, manage pain without heavy sedation, and your clinician confirms it’s safe (to reduce clot risk and manage complications). ERAS principles emphasize early mobilization; immobility works against recovery. [64]
If travel is unavoidable: plan aisle seating, hydration, walking breaks, and know where emergency surgical care is accessible along your route (a leadership lens on practical risk management). [76]
Public health and leadership reflections: why torsion is also a systems story
Ovarian torsion is the kind of condition that exposes the difference between “healthcare exists” and timely access to emergency surgery, anesthesia, imaging, and postoperative support. Global surgery literature and WHO messaging emphasize that billions of people lack access to safe, affordable surgical and anesthesia care when needed, an access gap that is ultimately measured in organs lost, disability, and preventable death. [77]
A women’s health advocacy frame is not only about awareness of symptoms, it’s also about strengthening emergency referral systems, respectful pain assessment, and clinical readiness to treat gynecologic emergencies decisively. The leadership question becomes: how do we build systems where a woman with acute pelvic pain is believed, evaluated rapidly, and treated promptly, regardless of geography, income, or institutional prestige? [78]
References
[1] [18] [22] [36] [37] [45] [80] Adnexal Torsion - Gynecology and Obstetrics - Merck Manual Professional Edition
[2] [6] [14] [15] [16] [17] [19] [21] [24] [38] [39] [40] [41] [47] [48] [55] [56] [71] Ovarian Torsion: Causes, Symptoms, Diagnosis & Treatment
[3] [4] [12] [27] [34] [35] [72] Adnexal Torsion in Adolescents: ACOG Committee Opinion No, 783 - PubMed
[5] [43] [91] Is unilateral oophorectomy associated with age at menopause? A population study (the HUNT2 Survey) - PubMed
[7] Ovarian Torsion | SAEM
[9] Ovarian Salvage With Prompt Surgical Intervention for Adnexal Torsion: Does Timing Matter? - PubMed
[10] Urgency of Evaluation and Outcome of Acute Ovarian Torsion in Pediatric Patients | Oncology | JAMA Pediatrics | JAMA Network
[11] Ovarian torsion: A retrospective case series at a tertiary care ...
[13] Ovarian torsion: A retrospective case series at a tertiary care center emergency department - PMC
[26] Pelvic Pain in Reproductive Age: US Findings - PMC
[33] The MRI whirlpool sign in the diagnosis of ovarian torsion - PMC
[46] [60] [64] Enhanced Recovery After Surgery (ERAS): New Concepts in the Perioperative Management of Gynecologic Surgery - PMC
[54] DIAGNOSTIC LAPAROSCOPY - PATIENT INFORMATION
[57] Nutrition and Wound Healing: An Overview Focusing on the ...
[58] A Patient's guide to Eating well before and after surgery
[59] Preventing pressure ulcers
[61] Opioid-Induced Constipation - StatPearls - NCBI Bookshelf
[63] Zinc in diet: MedlinePlus Medical Encyclopedia
[65] Recovering well after gynaecological laparoscopic surgery
[67] Laparoscopy: What to Expect at Home - My Health Alberta
[70] Prayer and pain: the mediating role of positive re-appraisal
[73] TIME'S A TICKIN': WHEN SHOULD SURGICAL ...
[74] Laparoscopy: What It Is, What To Expect & Recovery
[84] Biological Impact of Unilateral Oophorectomy - PMC - NIH
[86] Unilateral Oophorectomy and Age at Natural Menopause: A Longitudinal Community‐Based Cohort Study - PMC
[92] The influence of unilateral oophorectomy on the age of menopause - PubMed


Comments